Survival After SARD-ILD Exacerbation Differs by Race/Ethnicity
Why It Matters
The disparity underscores systemic barriers that reduce survival for minority SARD‑ILD patients, urging targeted interventions in outpatient management and transplant referral pathways.
Key Takeaways
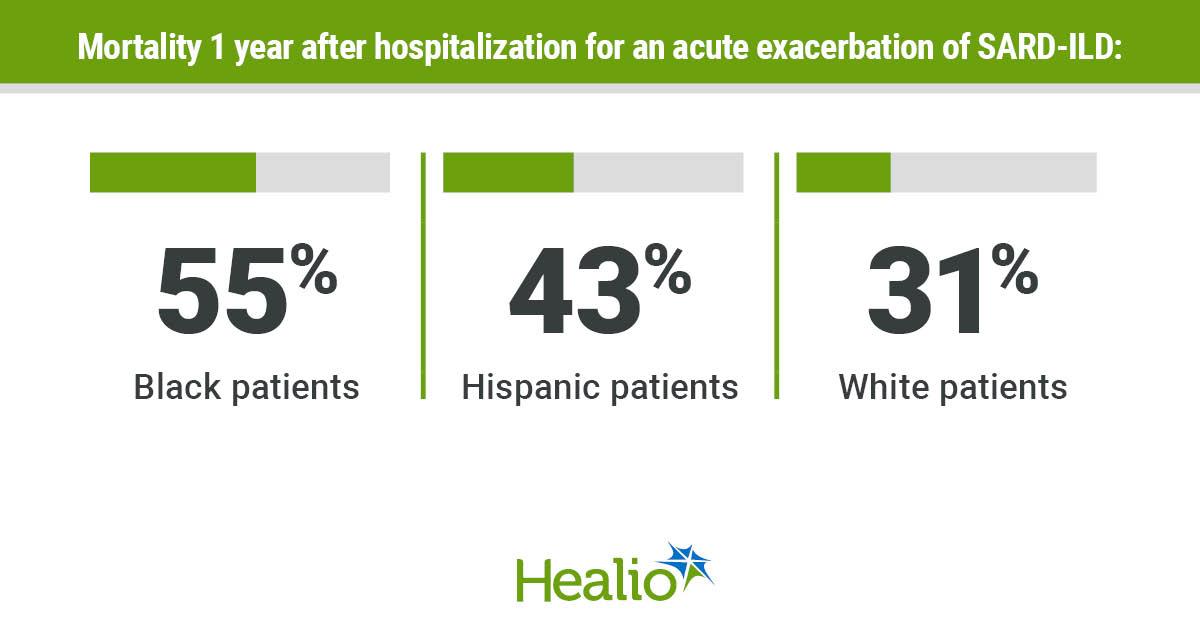
- •Black patients 55% 1‑year mortality after SARD‑ILD exacerbation
- •White patients comprised 46% of lung transplants, Black only 17%
- •No significant racial differences in in‑hospital mortality or ventilation
- •Study of 46 patients (2015‑2025) reveals post‑discharge survival gaps
Pulse Analysis
Systemic autoimmune rheumatic diseases such as systemic sclerosis, rheumatoid arthritis and mixed connective tissue disease often manifest with interstitial lung disease, a leading cause of morbidity. Acute exacerbations trigger rapid respiratory decline, frequently requiring intensive care and carrying high short‑term mortality. Understanding who is most vulnerable during and after these flares is essential for clinicians, payers, and policymakers aiming to improve outcomes in a disease that disproportionately burdens aging populations.
The recent analysis presented at the American Thoracic Society meeting examined 46 patients admitted between 2015 and 2025 at a major urban referral center. While in‑hospital outcomes—mortality, mechanical ventilation, ICU stay, and antifibrotic therapy—were statistically similar across racial groups, stark differences emerged after discharge. Black patients faced a 55% one‑year mortality rate, compared with 31% for white patients, and were far less likely to receive lung transplantation (17% versus 46% of transplants). These gaps point to inequities beyond the hospital walls, likely involving delayed referral, limited access to specialized transplant centers, and socioeconomic factors that affect follow‑up care.
The study adds to a growing body of evidence that health disparities in interstitial lung disease extend from diagnosis through advanced therapies. Addressing these gaps will require coordinated efforts: expanding culturally competent outreach, improving insurance coverage for high‑cost antifibrotic agents, and ensuring equitable transplant evaluation pathways. Future research should integrate socioeconomic data, geographic access, and gender analysis to pinpoint actionable levers. For health systems and advocacy groups, the message is clear—targeted policies and resource allocation are needed to close the survival gap and deliver equitable ILD care for all patients.
Survival after SARD-ILD exacerbation differs by race/ethnicity
Comments
Want to join the conversation?
Loading comments...