
Recent Posts
Social•Feb 22, 2026
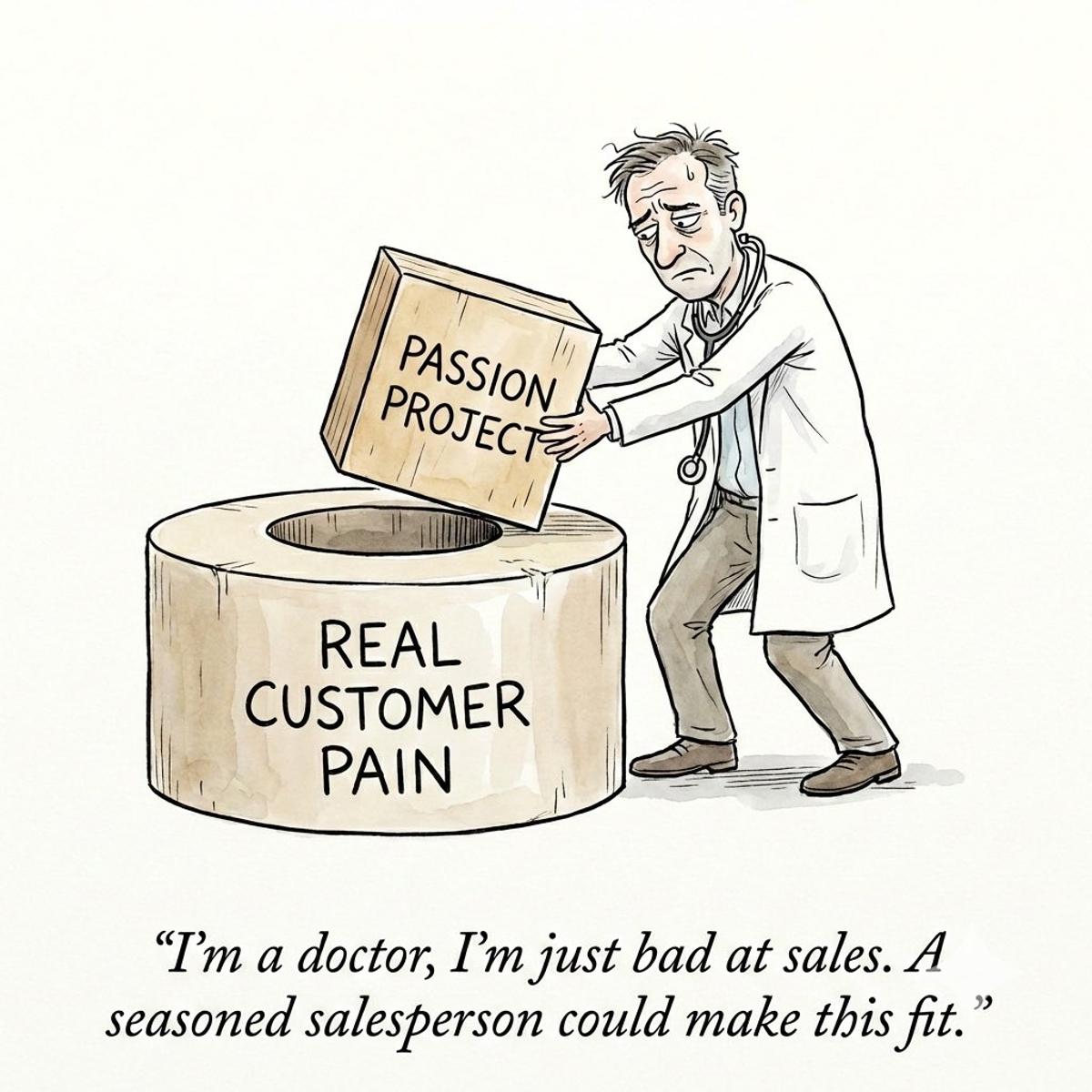
Clinician Startups Fail Because Product, Not Sales, Misses Market
When Clinician Entrepreneurs can’t get adoption, the Number 1 mistake is to think: “It’s not a product problem, it’s a sales problem.” Sorry but 99% of the time it IS a product problem. I’ve seen it over qnd over again from well-meaning clinician innovators. They: → Identify a clinical problem they are passionate about solving → Spend months (or years) just building the product and it works exactly as they imagined → Hustle their way to lots of meetings with potential customers. But besides them, no one else wants to use the product (and they definitely don’t want to pay for it) → Assume they are just bad at sales, so they spend lots of money hiring seasoned (ie expensive) sales people → The seasoned salespeople can’t sell it either → Entrepreneur eventually shuts down - but still walks away thinking “if only I had found the right sales person earlier” The truth is that if your innovation is truly solving a massive headache for many people - if Product - Market fit was truly there - sales shouldn’t be that hard. Yes, if you’re bad at sales, you will get less adoption than if you were good at it. But when your product has a true market, some customers desperate for a solution will adopt it anyways - despite how bad you are at sales. Think back to the start of the pandemic: how hard do you think it was to sell Zoom? The Clinician Entrepreneur should almost always be the 1st salesperson. If YOU - with all your passion and knowledge about the problem/product - can’t sell the first 10 customers, trust me, the best salesperson in the world can’t either. They can’t sell something that doesn’t have Product-Market fit, no matter how charismatic or brilliant they are. So if you can’t sell it, most likely the market for your product isn’t there (or is just really, really small). I’m sorry to say it but it’s probably true. So what do you do? You either pivot (the problem / product / market) to something with stronger market pull. Or you just keep working on your passion project, knowing that there just won’t be many adopters, but that’s fine with you because you built it first for yourself. But what you can’t do is keep spinning your wheels solving for the wrong thing in the adoption process.
By Joshua Liu, MD
Social•Feb 21, 2026
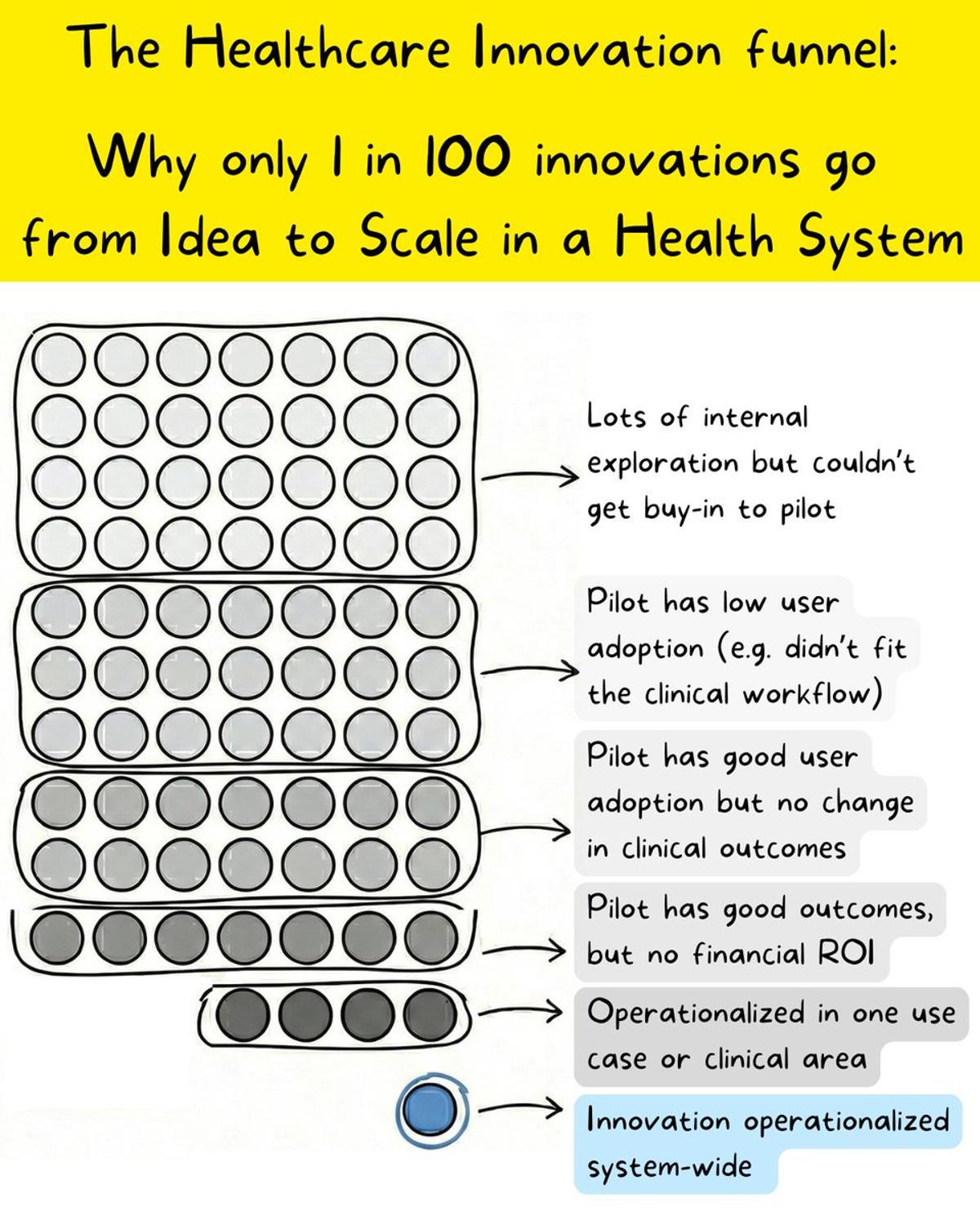
Most Health System Innovations Die Before Scaling
Many accuse health systems of not being willing to innovate. The truth? Lots of innovation is being explored all the time - you just don’t hear about them because most never make it to system-wide scale. For every 100 ideas that...
By Joshua Liu, MD
Social•Feb 21, 2026
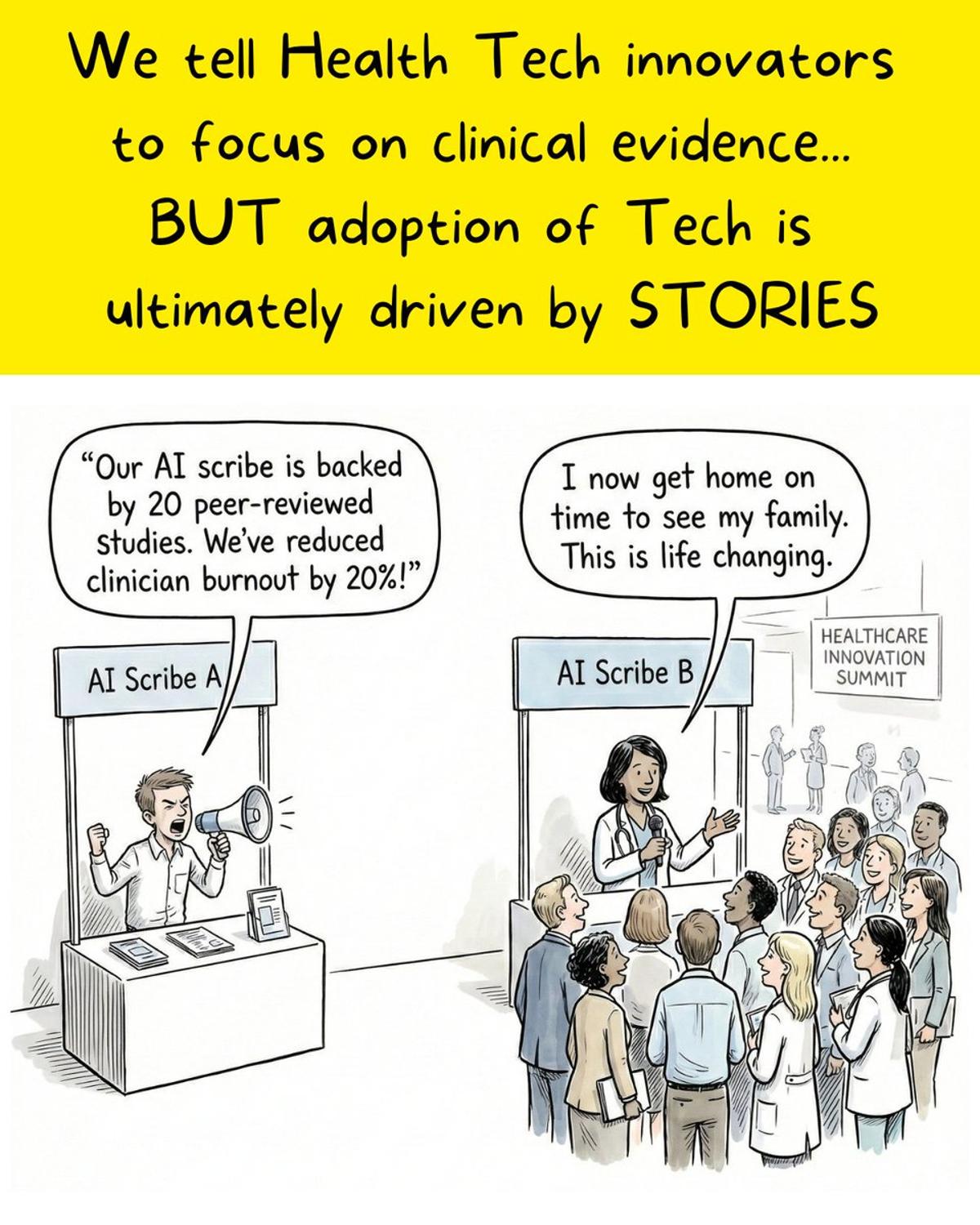
Stories, Not Data, Drive Health Tech Adoption
We want Health Tech to be evidence-based, but the truth is that adoption is ultimately driven by stories - NOT data. Here’s what I’ve seen play out over the past 13+ years over and over again: → Health system execs will choose...
By Joshua Liu, MD
Social•Feb 19, 2026
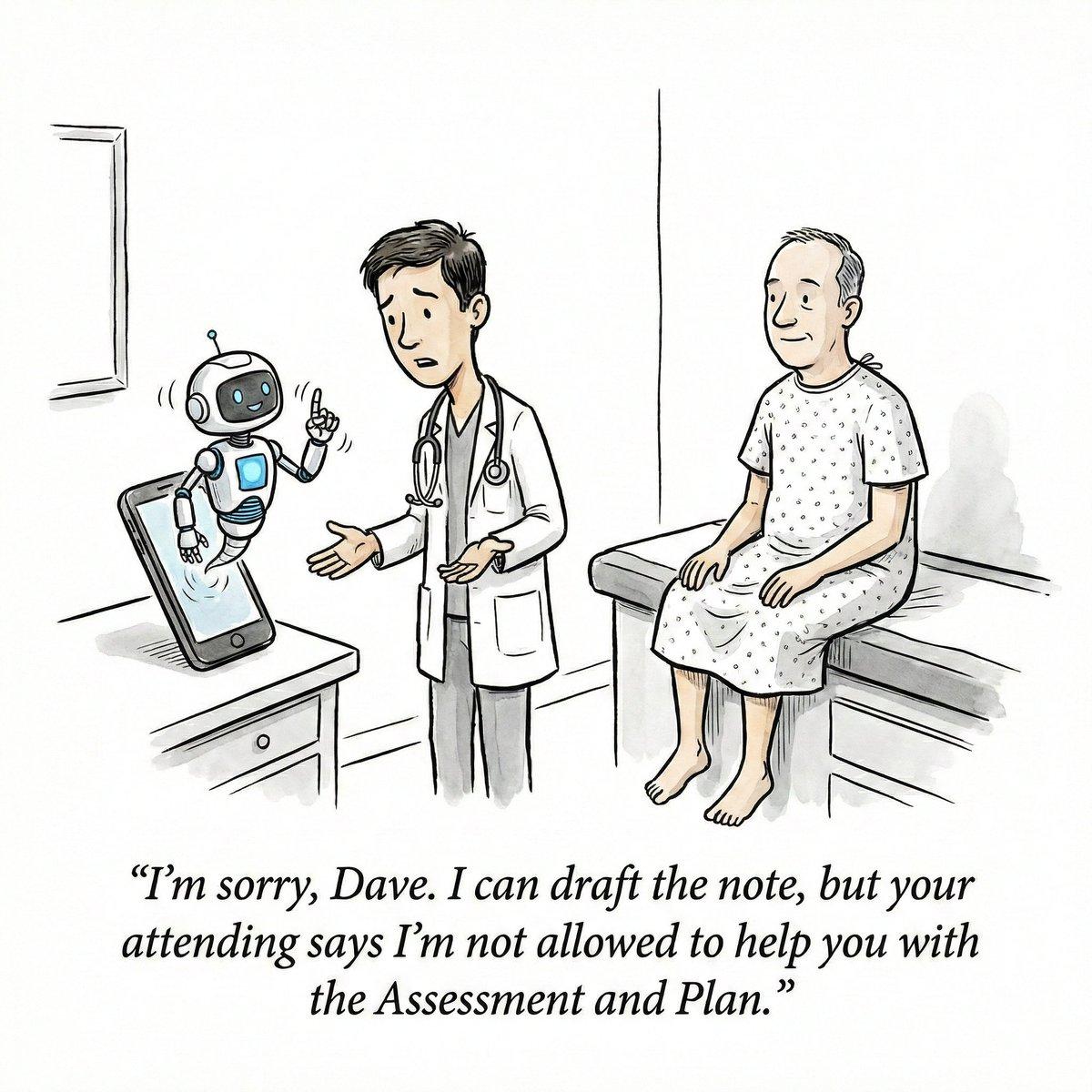
AI Scribes Should Aid Notes, Not Replace Trainee Assessments
Should residents and med students get access to AI scribes? Or does it risk critically de-skilling them? My 7 thoughts: 1/ Students are increasingly using scribes in all aspects of their life. I’m not in school anymore but I suspect many...
By Joshua Liu, MD
Social•Feb 17, 2026
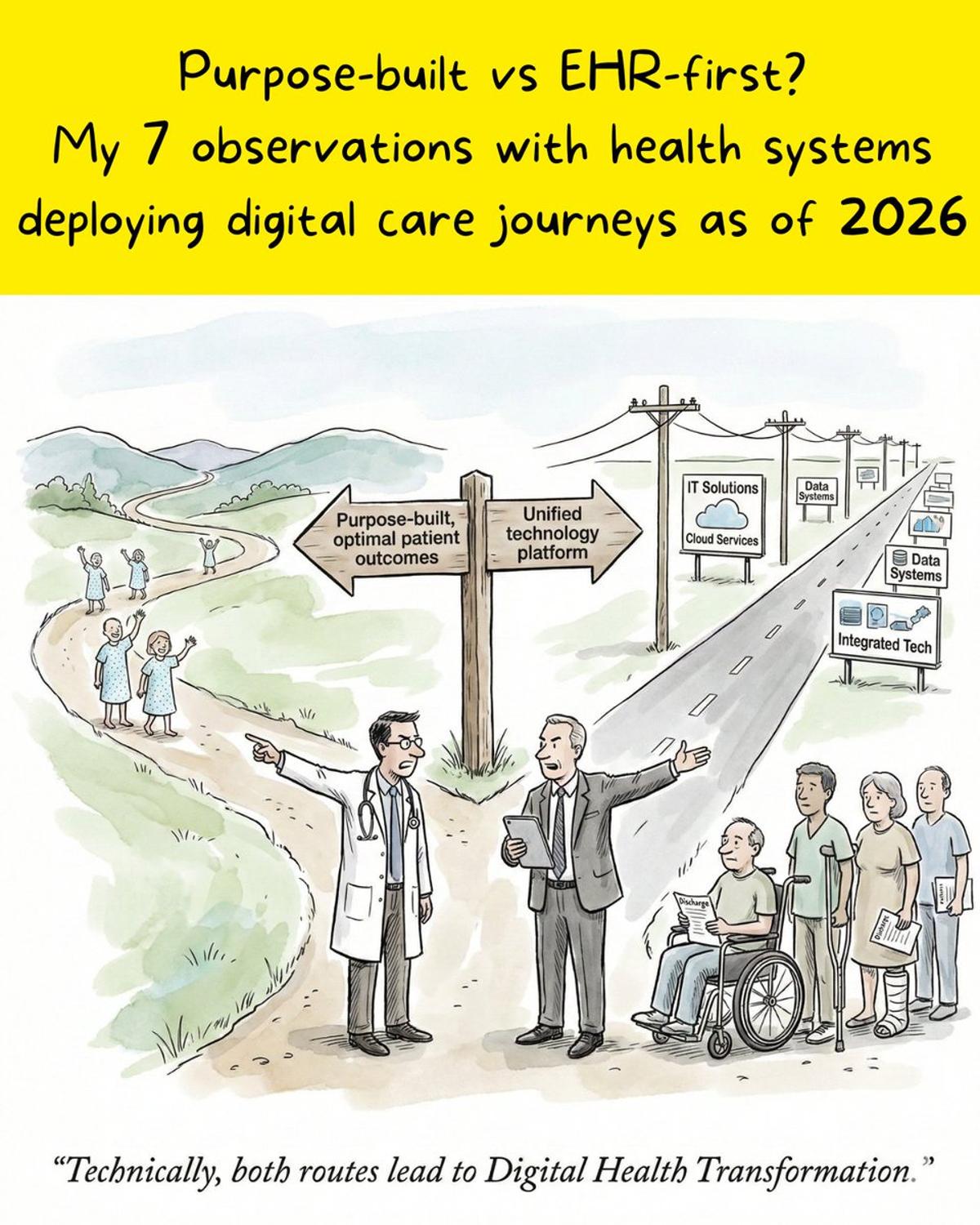
Executive Passion Drives Successful Digital Health Journeys
Since 2020, health systems have diverged in Digital Health strategies for patient journeys (e.g. pre/postsurgery engagement). Two main camps: Camp 1: “We will deliver the best digital experience for patients that delivers the highest patient adoption, engagement and outcomes - we’re...
By Joshua Liu, MD
Social•Feb 15, 2026
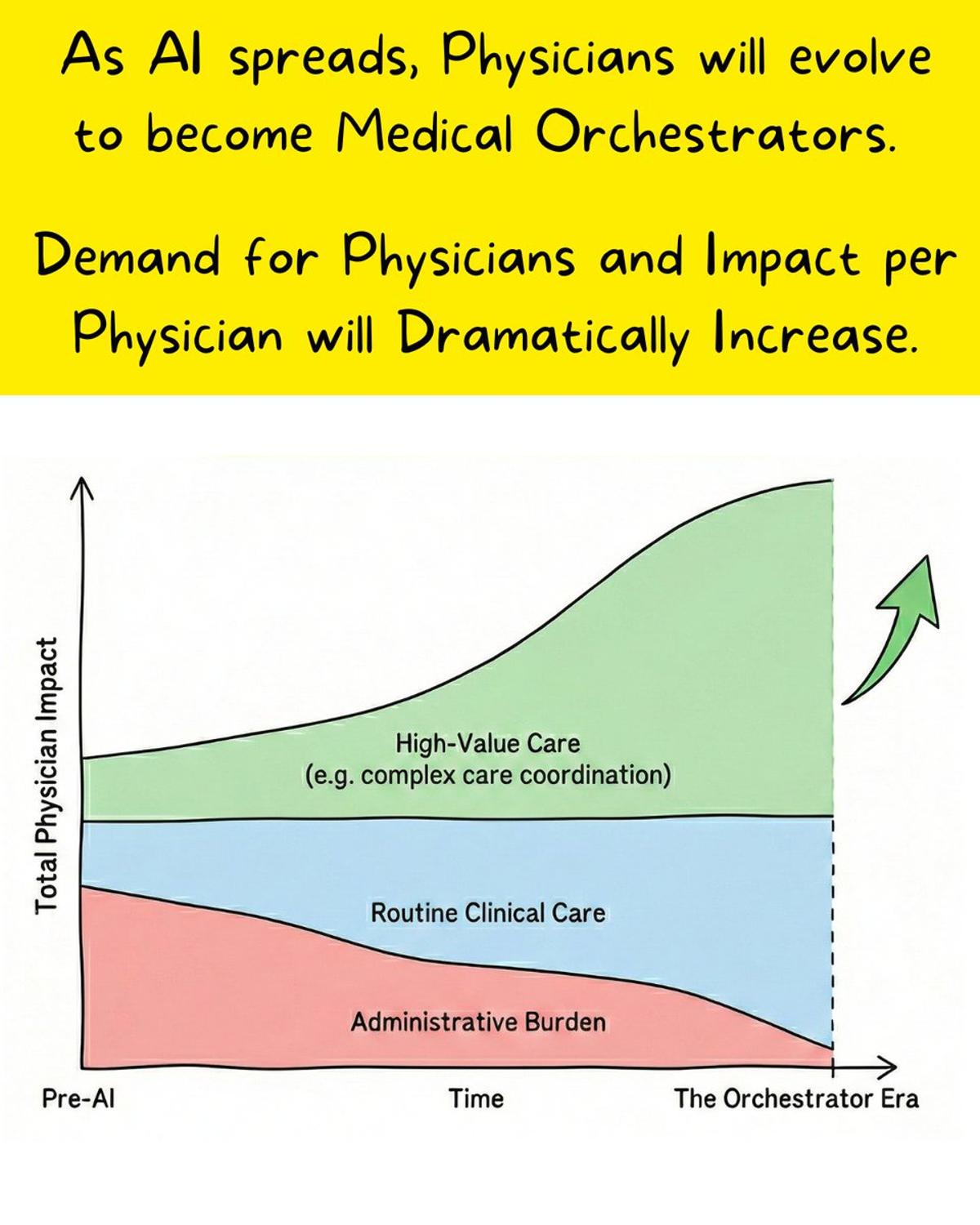
Physicians Evolve Into AI‑Guided Medical Orchestrators
Think AI will reduce demand for doctors? Consider this: Claude writes 100% of its own code, yet Anthropic's engineering team is exploding. We aren't looking at the end of the physicians, but the birth of Medical Orchestrators. When asked why Anthropic...
By Joshua Liu, MD
Social•Feb 14, 2026
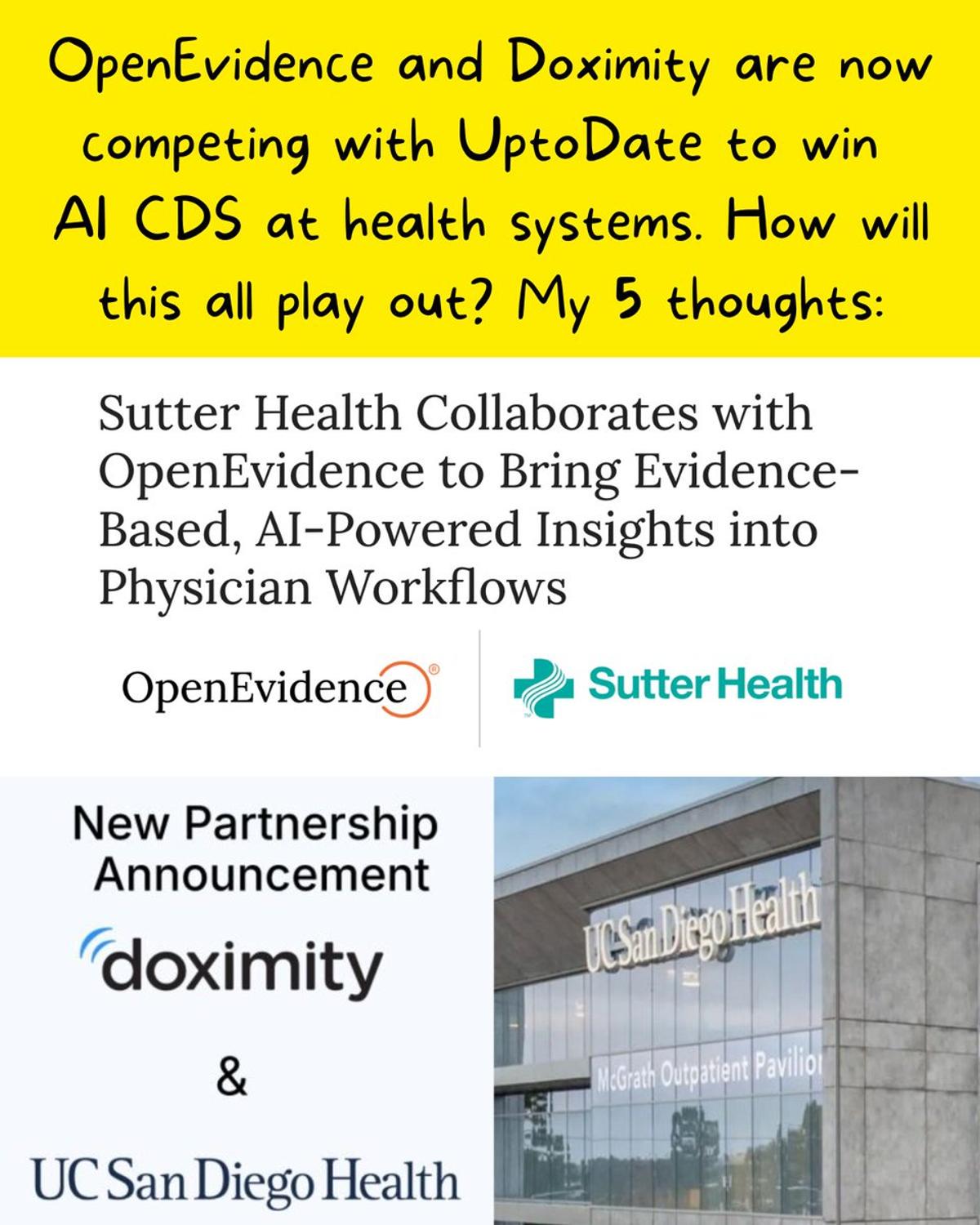
AI Docs Tools Expand Into Health System Enterprise
Those “direct-to-physician” CDS AI tools like OpenEvidence and DoximityGPT? They're now going after health systems too. My 5 thoughts on how this will all play out: First, the gist of what was announced: → Sutter Health will integrate OpenEvidence with Epic, allowing...
By Joshua Liu, MD