RW-ApoB -- Superior Metric For Lipid Related CVD Risk --- Using Lp(a), ApoB, and Triglycerides
Key Takeaways
- •RW‑ApoB outperforms LDL‑C, non‑HDL‑C, and apoB in CHD prediction
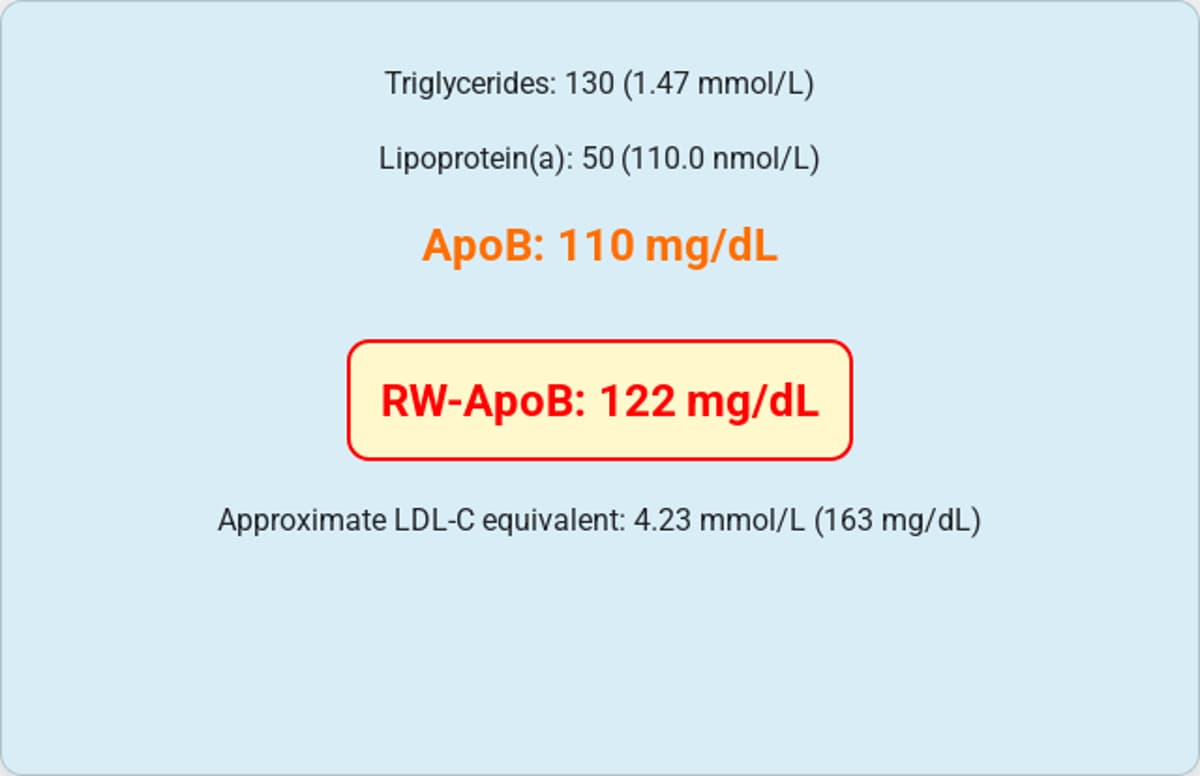
- •Formula: 11.65×TG + 0.215×Lp(a) + 0.736×ApoB
- •Study used 285,060 UK Biobank participants not on lipid therapy
- •Model discounts raw ApoB, yielding values below measured ApoB
- •Non‑fasting TG and fixed Lp(a) conversion inflate risk estimates
Pulse Analysis
Traditional lipid panels rely on LDL‑C or non‑HDL‑C to gauge atherogenic burden, yet these metrics ignore the full spectrum of apoB‑containing particles. ApoB itself counts the number of potentially harmful lipoproteins, but it still overlooks the heightened risk posed by triglyceride‑rich remnants and lipoprotein (a). As cardiovascular disease remains the leading cause of death in the United States, clinicians and researchers are seeking a more inclusive risk score that captures all atherogenic contributors without adding complexity to routine testing.
The RW‑ApoB metric attempts to fill that gap by assigning weighted coefficients to triglycerides, Lp(a), and apoB, producing a single number that reflects the combined risk of LDL, TRL/remnants, and Lp(a). In a massive UK Biobank cohort of over 285,000 individuals free of lipid‑lowering therapy, RW‑ApoB showed superior CHD prediction accuracy compared with LDL‑C, non‑HDL‑C, and apoB alone. The study’s authors calibrated the formula so that the median RW‑ApoB matches the median measured apoB, a choice that improves population‑level fit but forces the apoB coefficient below one, causing RW‑ApoB to dip beneath raw apoB values in low‑risk subjects.
Critics highlight several methodological concerns: the use of non‑fasting triglyceride measurements, a fixed conversion factor for Lp(a) that can misrepresent true particle concentration, and the exclusion of low‑apoB participants from validation cohorts. These choices may artificially boost the metric’s apparent performance while obscuring its mechanistic interpretation. For the metric to gain clinical traction, future iterations should ensure RW‑ApoB never falls below measured apoB, incorporate fasting triglyceride data, and apply isoform‑specific Lp(a) conversions. Until then, RW‑ApoB remains a promising but imperfect tool for refining cardiovascular risk assessment.
RW-ApoB -- Superior Metric For Lipid Related CVD Risk --- Using Lp(a), ApoB, and Triglycerides
Comments
Want to join the conversation?