Weird Health Insurance Concepts | Out-Of-Pocket
•March 11, 2026
0
Key Takeaways
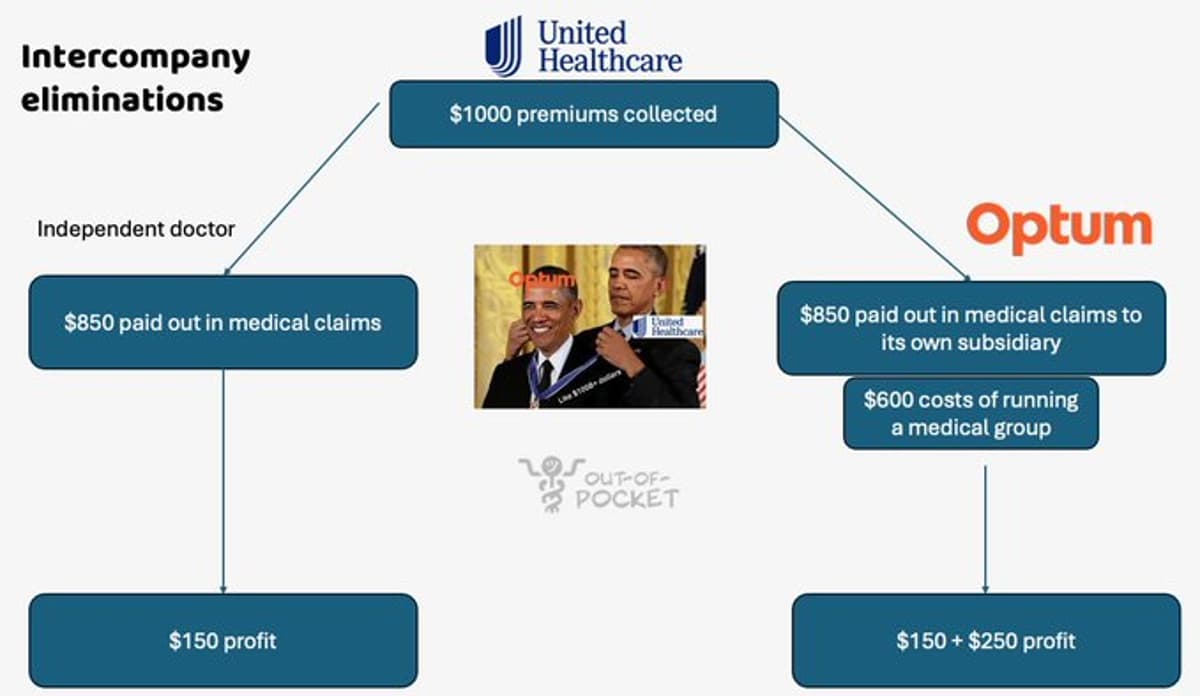
- •Intercompany eliminations let insurers count subsidiary payments toward loss ratios
- •Copay accumulators block manufacturer coupons from meeting deductibles
- •Copay maximizers inflate patient copays to increase pharma assistance
- •Reference-based pricing ties reimbursement to Medicare rates, limiting costs
- •RBP can generate surprise bills when providers reject payer rates
Summary
The article explains three emerging health‑insurance tactics—intercompany eliminations, copay accumulators/maximizers, and reference‑based pricing—that reshape cost flows and patient liabilities. Intercompany eliminations let insurers count payments to owned providers toward medical loss‑ratio requirements, effectively boosting margins. Copay accumulators prevent manufacturer coupons from satisfying deductibles, while maximizers inflate patient copays to increase pharma assistance. Reference‑based pricing reimburses a fixed percentage of Medicare rates, offering price transparency but exposing patients to balance‑billing risks.
Pulse Analysis
Intercompany eliminations have become a cornerstone of vertical integration in the U.S. health‑insurance market. By treating payments to owned physician groups, PBMs, or specialty pharmacies as internal cost offsets, insurers can meet the 85 % medical loss‑ratio threshold while retaining a larger share of premium revenue. This accounting maneuver not only improves reported profitability but also creates incentives to steer patients toward in‑network, captive providers, potentially squeezing independent clinics out of the market.
Pharmaceutical manufacturers have responded to rising out‑of‑pocket burdens with copay assistance programs, prompting insurers to deploy two counter‑strategies. Copay accumulators exclude manufacturer coupons from deductible calculations, forcing patients to shoulder the full deductible before assistance applies. Conversely, copay maximizers artificially raise the patient’s share, prompting the manufacturer’s program to cover a larger amount. Both tactics reshape the cost‑sharing landscape, shifting financial pressure between insurers, drug makers, and consumers while complicating claims processing.
Reference‑based pricing (RBP) offers a different approach by anchoring reimbursements to a known benchmark—typically a percentage of the Medicare rate. Employers using self‑insured plans appreciate the predictability and potential savings, as RBP eliminates the need for complex provider negotiations. However, the model can generate surprise balance‑bills when providers reject the payer‑set rate, leading to disputes and administrative overhead. As more employers experiment with RBP, regulators and insurers must balance cost containment with patient protection to avoid unintended financial shocks.
Comments
Want to join the conversation?