Hospitals, Insurers Clash on 340B Rebate Costs
Why It Matters
The 340B rebate model could reshape drug‑pricing dynamics; its cost assumptions will determine whether hospitals absorb billions in new expenses or manufacturers avoid costly duplicate discounts, influencing overall healthcare spending.
Key Takeaways
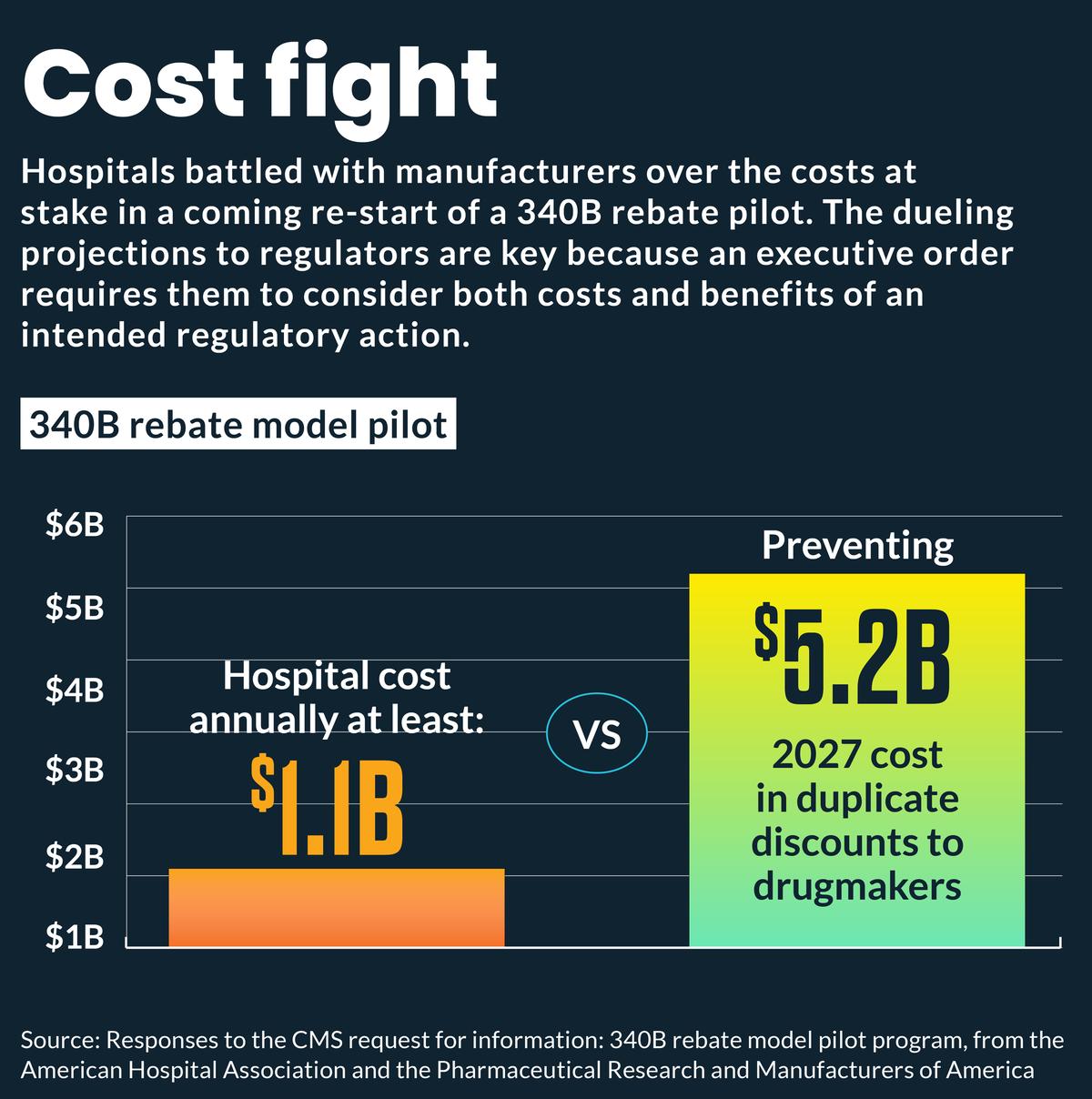
- •AHA estimates $1.15 billion annual cost to run 340B rebate model
- •Hospitals would need one full‑time pharmacist per site, costing $750 million
- •PhRMA argues rebate model could save manufacturers $5.23 billion in 2027
- •Float payments could cost individual hospitals up to $300 k annually
- •Regulators face conflicting cost projections as they consider 340B rebate pilot
Pulse Analysis
The 340B Drug Pricing Program, created in 1992, allows eligible hospitals to purchase outpatient drugs at steep discounts, helping offset the cost of caring for low‑income patients. HRSA’s recent request for information signals a potential shift from the traditional discount model to a rebate‑based system that would require manufacturers to return a portion of sales after the fact. Proponents argue that a rebate could close loopholes that enable duplicate discounts under the Inflation Reduction Act and Medicaid, while critics fear it adds administrative complexity and financial strain.
Hospital advocates, spearheaded by the American Hospital Association, have quantified the financial burden of the proposed rebate. Their analysis projects more than $1 billion in annual expenses nationwide, driven by the need to hire a full‑time pharmacist at each of the 2,728 participating facilities—an estimated $750 million—and additional operational costs of roughly $400 million. Individual institutions anticipate administrative outlays ranging from $150,000 to $1.5 million, with float costs—delays in reimbursement—potentially adding another $300,000 per hospital. These figures raise concerns that the rebate could outweigh any savings from reduced duplicate discounts.
Pharmaceutical manufacturers, represented by PhRMA, contend that the rebate model would generate substantial savings by eliminating duplicate discounts that currently cost the industry billions. They estimate $5.23 billion in avoided duplicate discounts in 2027 alone, plus $1.5 billion in overlapping Medicaid discounts. If implemented, the rebate could provide a transparent mechanism for reconciling 340B and other federal pricing programs, potentially lowering overall drug spending. Regulators must now weigh these competing cost‑benefit narratives, as the outcome will influence hospital cash flow, manufacturer pricing strategies, and the broader trajectory of federal drug‑price reforms.
Hospitals, insurers clash on 340B rebate costs
Comments
Want to join the conversation?
Loading comments...