Tile-Based Radiation Improves Outcomes for Brain Metastases
Companies Mentioned
Why It Matters
The data position intra‑operative tile therapy as a faster, more effective alternative to stereotactic radiosurgery, promising improved disease control and survival for patients with resected brain metastases.
Key Takeaways
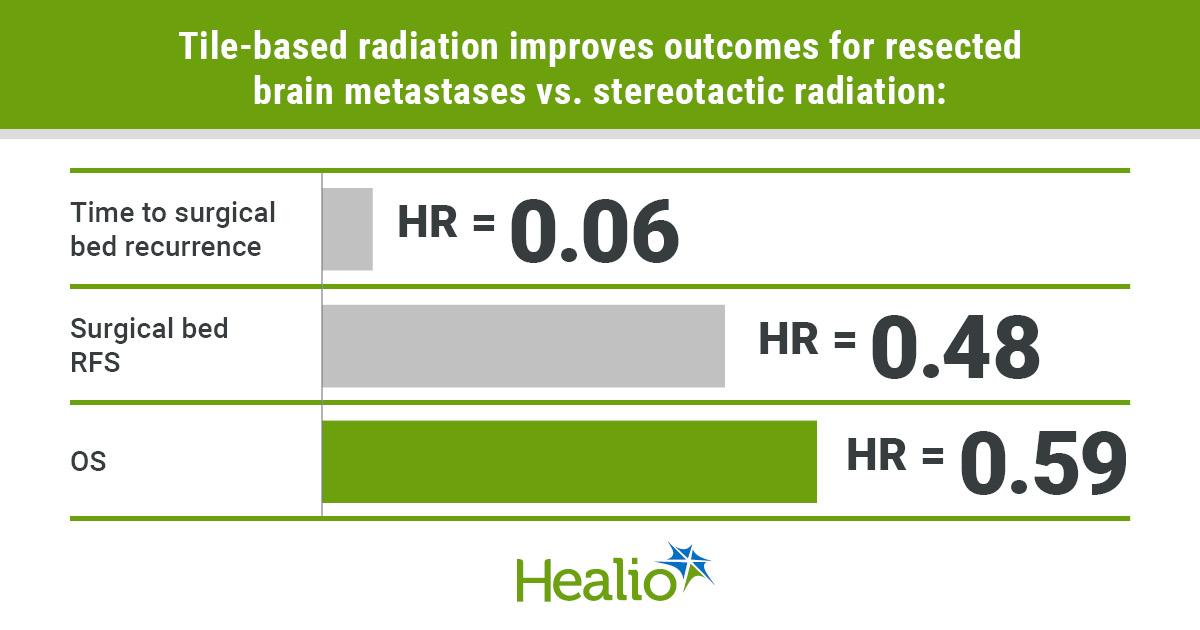
- •Tile therapy cut 12‑month recurrence to 1.3% vs 15.4% with stereotactic.
- •Overall survival at 24 months rose to 61.7% versus 35.7%.
- •Radiation delivered intraoperatively, reducing time to completion from 30 to 1 day.
- •Adverse event rates similar between tile and stereotactic arms.
- •Phase 3 trial enrolled 204 patients across multiple centers, confirming efficacy.
Pulse Analysis
Brain metastases affect roughly one‑third of patients with advanced solid tumors, and surgical resection followed by postoperative radiation has become the de‑facto standard. Conventional stereotactic radiosurgery (SRS) is typically scheduled weeks after surgery, creating a window where residual microscopic disease can proliferate and where logistical hurdles may prevent patients from completing treatment. Moreover, the steep dose gradients of SRS can limit the total energy delivered to the resection cavity, potentially compromising local control.
Cesium‑131 tile‑based brachytherapy addresses these gaps by adhering radiative tiles directly to the cavity wall at the end of the operation. The high‑energy, short‑half‑life isotope delivers a concentrated 100‑120 Gy dose to the immediate margins while sparing deeper brain tissue, and it releases roughly 90% of that dose over a six‑week period. The phase‑3 trial’s hazard ratios—0.07 for recurrence and 0.59 for overall survival—demonstrate a dramatic advantage, especially given the comparable safety profile. Immediate implantation also eliminates the typical 30‑day lag to radiation, a factor that previously left up to 20% of patients without definitive postoperative therapy.
If adopted widely, tile‑based therapy could reshape neuro‑oncology workflows, allowing surgeons and radiation oncologists to coordinate care in a single operative session. The streamlined approach may lower overall treatment costs by reducing repeat imaging and multiple appointments, while the improved local control could enable patients to maintain systemic therapies longer without interruption. Ongoing studies will need to confirm long‑term survival benefits and explore applications beyond resected metastases, such as primary glioblastoma, but the current evidence positions cesium‑131 tiles as a compelling candidate for the next standard of care.
Tile-based radiation improves outcomes for brain metastases
Comments
Want to join the conversation?
Loading comments...